
Radial Head Subluxation (Nursemaid’s Elbow)
Written by: Andrew Shanes, DO; Edited by: Timothy Khowong, MD, MSED
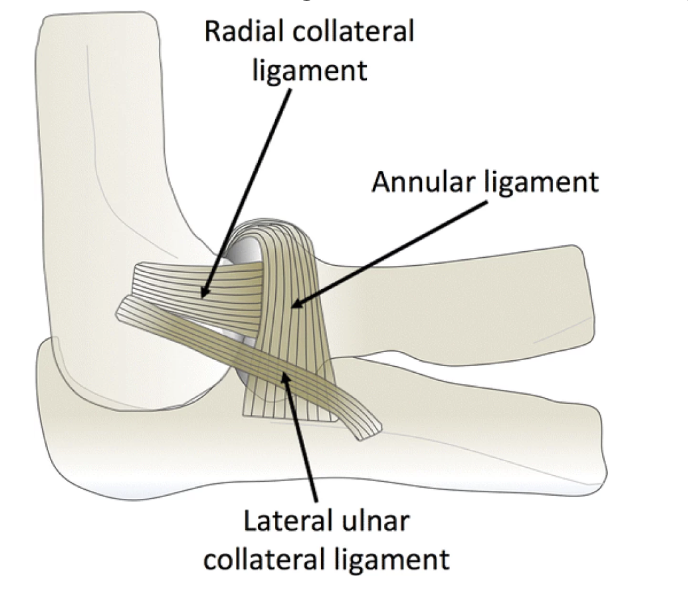
Anatomy Review:
There are 3 Main Ligaments of the lateral elbow: Lateral Ulnar Collateral Ligament, Radial Collateral Ligament, and the Annular Ligament.
How does it occur?
Nursemaid’s elbow occurs when the radial head gets “pulled” out from the annular ligament due to sudden, longitudinal traction that applied to the hand with the elbow extended. It is most common in children from 1 to 4 years of age (average age is 28 months) as joints and ligaments in young children are still growing and are relatively loose.
Common mechanisms: lifting a child by the hand, swinging a child around, grabbing a child to stop a fall, picking up a kid off the ground, pulling an arm out of a jacket.
What happens?

The longitudinal traction force causes the radial bone to start moving out of place and gets stuck on the annular ligament fibers, causing the annular ligament to become interposed between radial head and capitellum.
After age 5, the distal attachment of the annular ligament starts to become thicker and stronger, helping prevent subluxation in older children
Patient Presentation
Child refuses to use the arm with his/her arm held in slight flexion. Patients tend to have no tenderness to direct palpation but can have pain with forearm supination or movement of the elbow.
Patient Management
If the history and examination are strongly suggestive, radiographs are not needed and reduction can be performed. However, if the history is atypical or there is point tenderness/signs of trauma, radiographs should be obtained.
Reduction Techniques
Reduction can be performed via one of two techniques: Supination-Flexion or Hyperpronation. Techniques are shown below.

Supination-Flexion



Hyperpronation


Comparison of Reduction Techniques
A Systematic Review looked at 7 Randomized Trials that included 701 patients (350 treated with the hyperpronation maneuver versus 351 patients who underwent the supination-flexion maneuver). Meta-analysis showed that hyperpronation was more effective than supination-flexion (risk ratio, 0.34; 95% confidence interval, 0.23 to 0.49; I2, 35%) with an absolute risk difference between maneuvers was 26.4%, and a Number Needed to Treat of 3.8, meaning for every 4 children treated with Hyperpronation, rather than Supination-Flexion, for nursemaid's elbow, there will be one less failure at first reduction attempt.
The quality of evidence was low, and susceptibility to bias was high, in all of the studies due to the impossibility of blinding subjects, providers, and assessors after allocation of treatment intervention.
A second study which was a Randomized Control Trial that assessed 116 patients with 60 patients treated with supination-flexion technique and 56 patients treated with hyperpronation technique.In the supination-flexion group, 53.33% of patients were properly reduced after the first attempt, while in the hyperpronation group, 85.71% patients were reduced in the first attempt.
These studies did include some limitations including the inability to blind subjects and providers to the treatment intervention, as well as inability to quantify the time since injury and what impact that had on the success of the reduction. However, overall the significant difference favoring hyperpronation technique to supination-flexion in these studies show great consideration that hyperpronation should be performed as a the first attempt reduction technique in treating Nursemaid’s Elbow.

Other Considerations
If the history is atypical or there is point tenderness or signs of trauma, radiographs should be obtained.
Ultrasound can be helpful for confirming the diagnosis when the mechanism of injury is not evident or when physical examination is inconclusive.
On ultrasound, one can see an increased prominence of the synovial fringe which appears to fall into the joint space between capitellum and radial head, and look more pointed. While this has a sensitivity 64.9% and specificity 100%, if there is concern for other injury/signs of trauma/tenderness, x-rays should be obtained as well.

Recurrence/Prevention
Recurrence is very high for children with nursemaids' elbow injury due to ligamentous laxity and recurrent pull injury. Some studies estimate it between 27% to 39%, but up to 62.5% in some patients.
Parents should be educated to not forcefully pull/jerk or swing their child by the arm or hands. There should be an emphasis placed on the importance of using verbal cues instead of physical actions to get your child’s attention and to be patient with young children putting their arms through jackets and climbing into car seats.
Resources
Ulici A, Herdea A, Carp M, Nahoi CA, Tevanov I. Nursemaid's Elbow - Supination-flexion Technique Versus Hyperpronation/forced Pronation: Randomized Clinical Study. Indian J Orthop. 2019 Jan-Feb;53(1):117-121. doi: 10.4103/ortho.IJOrtho_442_17. PMID: 30905991; PMCID: PMC6394198.
Rens Bexkens, Frederic J. Washburn, Denise Eygendaal, Michel P.J. van den Bekerom, Luke S. Oh. Effectiveness of reduction maneuvers in the treatment of nursemaid's elbow: A systematic review and meta-analysis. The American Journal of Emergency Medicine, Volume 35, Issue 1, 2017, Pages 159-163, ISSN 0735-6757, doi: 10.1016/j.ajem.2016.10.059.
Grace O'Neill, Wiiliam Hennrikus; Recuurence rate in Nursemaid's Elbow in Children. Pediatrics August 2019; 144 (2_MeetingAbstract): 752. 10.1542/peds.144.2MA8.752
Ichwan, D. (2021) Emrad: Can’t miss pediatric elbow injuries, ALiEM. Available at: https://www.aliem.com/emrad-ped-elbow-cant-miss/
Lustosa L, Knipe H, Carroll D, et al. Pulled elbow syndrome. Reference article, Radiopaedia.org https://doi.org/10.53347/rID-15748
Cicero MX. Musculoskeletal Disorders in Children. In: Cydulka RK, Fitch MT, Joing SA, Wang VJ, Cline DM, Ma O. eds. Tintinalli's Emergency Medicine Manual, 8e. McGraw-Hill Education; 2017. https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2158§ionid=162271497
Shaath, K. and Shirley, E. (2022) Nursemaid’s elbow, Orthobullets. Available at: https://www.orthobullets.com/pediatrics/4012/nursemaids-elbow
Yamanaka S, Goldman RD. Pulled elbow in children. Can Fam Physician. 2018 Jun;64(6):439-441. PMID: 29898933; PMCID: PMC5999240.