
Snapping the Scapula
Written by Jing Jing Gong, MD; Edited by Timothy Khowong, MD

Image 1: “Hand to shoulder sign,” which suggests that an anime character is in pain. Pictured above is Light Yagami from animated series, Death Note
Case presentation
You are working a busy overnight shift in the ER, and you encounter a 41 year-old man who presents to the emergency room via EMS due to right shoulder pain after he lost control of his motorcycle 7 hours ago. Patient was wearing a helmet; while he was trying to exit the highway he slipped on gravel while traveling 20-30 mph. He stated he fell onto his left side and now has left-sided shoulder pain. You decide to obtain a shoulder X-Ray.
What imaging views would you like to obtain?
Anatomy of the scapula
The scapula is a triangular-shaped bone that articulates with the clavicle at the acromioclavicular joint, with the humerus at the glenohumeral joint, and with the thorax at the scapulothoracic joint. Together, the scapula, humerus, and thorax allow for upper extremity range of motion. These include elevation, depression, protraction, retraction, and rotation of the shoulder. When scapular fractures occur, approximately 50% involve the body and spine of the scapula.
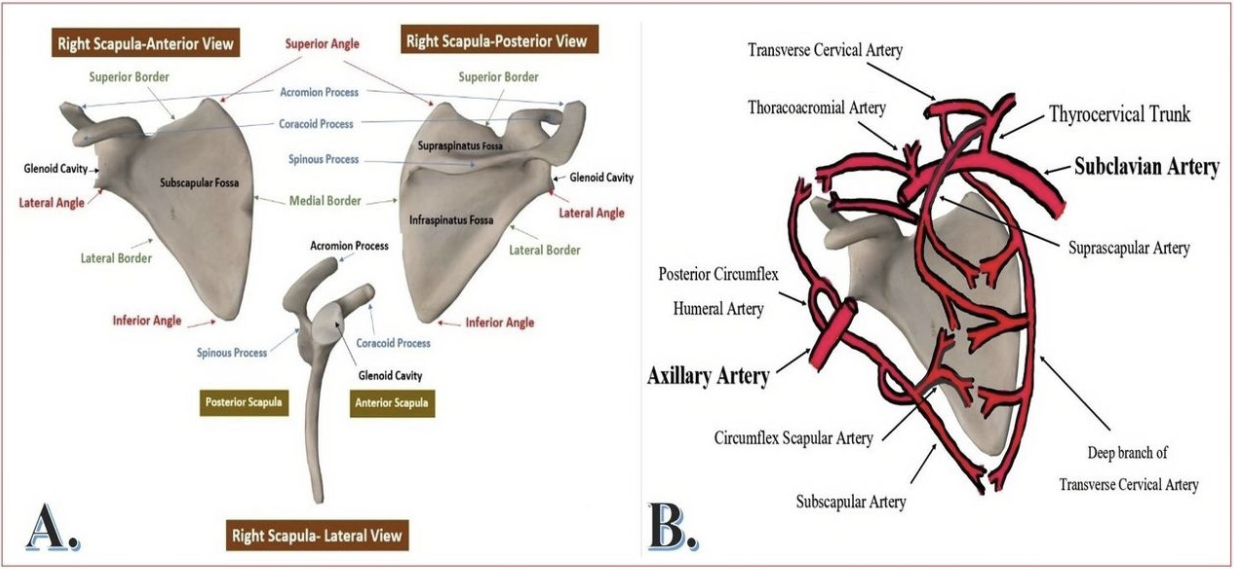
Image 2: Anatomy of the scapula (left) and surrounding vasculature (right)
Imaging
Below are the X-Ray images obtained; can you identify the fracture?




Image 3: X-rays obtained of patient’s left shoulder demonstrating vertical scapula fracture of the body. Four view obtained: (A) AP view with internal rotation; (B) AP view with external rotation; (C) Scapular Y-View; (D) Axillary view
Once scapular fracture is identified on X-ray, the standard of care is to obtain a CT scan.

Image 4: CT scan of the patient’s left shoulder demonstrating mildly displaced left scapular fracture in axial view
The X ray images demonstrate a clear linear, vertical radiolucency in the scapula body that suggests a scapular fracture. This is better delineated on CT scan, which was obtained to assess for any subluxation or displacement of the glenoid. CT imaging is also useful for identifying additional fractures along the scapula involving the coracoid process or the acromion process.
In our patient, CT scan (Figure 2) revealed that the only site of acute injury was the scapular body with no evident injury to the glenoid, acromion process, or the coracoid process.
Physical Exam Findings
Patients who present with scapular fracture often present with an adducted arm, edema, ecchymosis, and tenderness. Active range of motion will be limited across all planes secondary to pain.
Vascular capillary refill, brachial pulse, and nerves originating from brachial plexus including the suprascapular nerve and axillary nerves should also be evaluated.
Scapular Fracture Classification
Multiple scapular fracture classification systems exist. The primary method of stratification is based on anatomic site of injury. Here, we explore the classification system from Orthopedic Trauma Association (OTA).
Based on the OTA classification, there are 3 primary types of scapula fractures: extra-articular (not involving glenoid), partial articular (partial involvement of glenoid), and total articular (complete glenoid involvement).
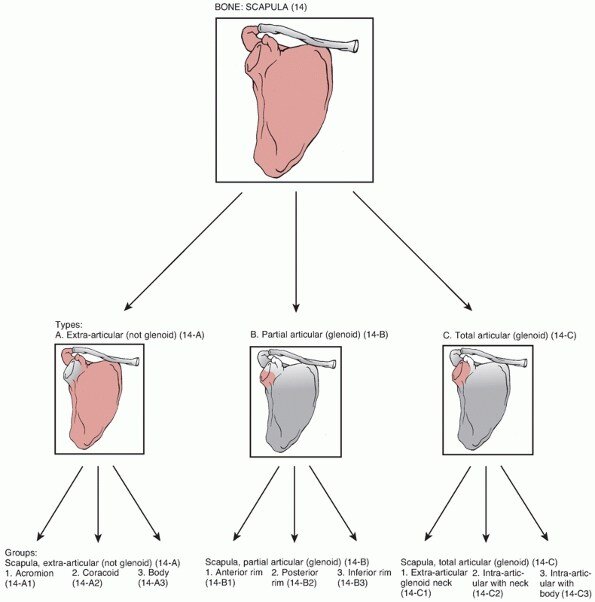
Image 5: The OTA classification system of scapular fractures (image from teachmeorthopedics, 2021)
Associated Injuries:
What are the associated traumatic injuries of scapula fracture?
Patients who present to ER for high-energy mechanism injuries are at increased risk of scapular fractures. While scapula fractures account for less than 1% of all fractures, 80-90% of such cases have associated injuries.
What are the medically associated injuries?
Patients who have sustained scapular fracture injuries are also found to have medically associated injuries including the following: pulmonary contusion (41%), pneumothorax (32%), head injury (35%), and vascular injury (11%).
Treatment
The treatment regimen for minimally displaced scapula fractures are primarily non-operative. These patients can wear a sling for 2 weeks while conducting early motion rehabilitation exercises. Most patients experience union in approximately 6 weeks with no functional deficits identified.
When Should Orthopedics Be Consulted?
Patients will require orthopedic surgery if there are physical exam findings or CT findings of glenohumeral instability. If there is greater than 25% of glenoid involvement, >5 mm glenoid articular displacement, or is an open fracture, patients will also require surgery. Orthopedics team should be involved for follow-up if the patient qualifies for conservative management.
References:
Cowan PT, Mudreac A, Varacallo M. Anatomy, Back, Scapula. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531475/
Dupaix JP, Opanova MI, Elston MJ, Lee LSK. A Comparison of Skeletal Injuries Arising from Moped and Motorcycle Collisions. Hawaii J Health Soc Welf. 2019;78(10):311-315.
Marsh JL, Slongo TF, Agel JNA, et al. Fracture and dislocation classification compendium —2007: Orthopaedic Trauma Association classification, database, and outcomes committee. J Orthop Trauma 2007;21:S1-S6.
https://teachmeorthopedics.info/scapular-fractures/
https://radiopaedia.org/articles/scapular-fracture?lang=us
https://www.orthobullets.com/trauma/1013/scapula-fractures